
Rupture of the cranial cruciate ligament (CrCL) is one of the most common orthopedic problems in dogs. The condition mostly affects medium, large and giant breed dogs and especially active, overweight dogs. However, more often than direct trauma, the cause of cranial cruciate ligament rupture is its progressive degeneration as a result of chronic loading with coexisting anatomical, autoimmune, hormonal factors, etc. Chronic inflammation of the cranial cruciate ligament, manifested by temporary lameness, leads to its partial, and eventual, full rupture. The condition is increasingly diagnosed in representatives of miniature breeds.
Instability in the femoral-tibial joint is characterized by the occurrence of significant discomfort and a high degree of lameness and leads to a number of degenerative changes in the joint, damage to the articular cartilage, the meniscus, as well as the formation of degenerative reactions limiting mobility in the joint.
Surgical treatment aims to achieve stability of the stifle joint, remission of clinical symptoms and prevention of progressive degeneration of the joint.
The most commonly used surgical techniques include arthroscopic stabilization by Flo, TightRope, TTA with modifications, TPLO, CBLO, CTWO.
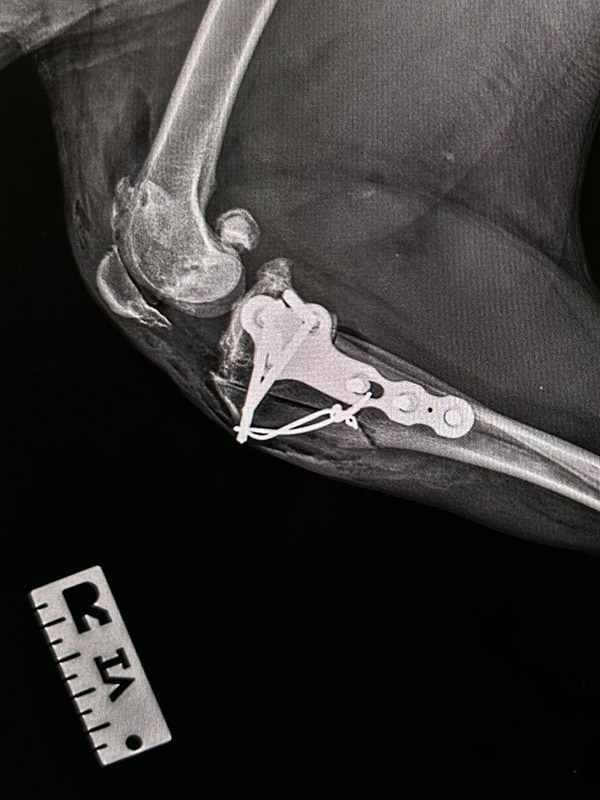
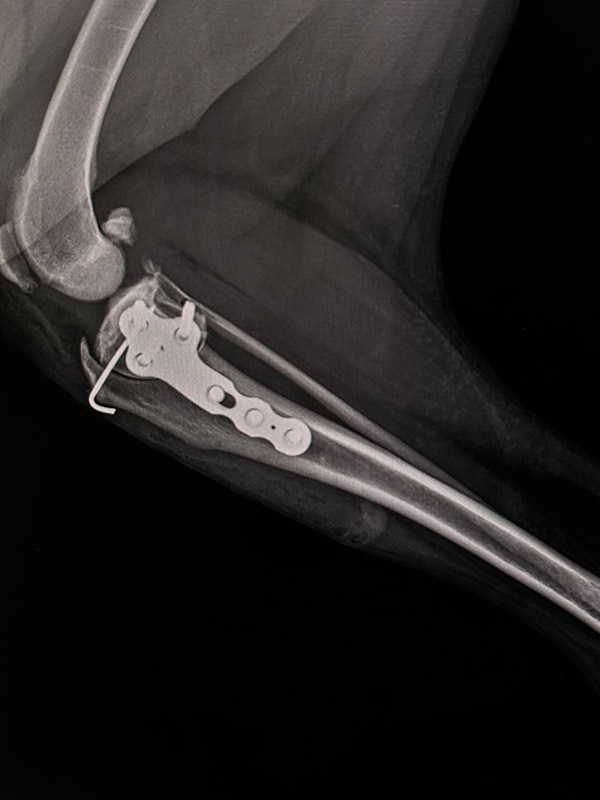
In miniature breeds, the most commonly accepted method of CrCL repair is stabilization with a tibiofibular suture using non-absorbable suture material or ready-made prostheses such as SMI or Arthrex FiberWire. However, more and more often in clinical practice, we encounter complications that make this method unsatisfactory. Extracapsular stabilization does not take into account the degree of tibial plateau plane angle, which in a large percentage of these breeds is higher than the standard average of 18- 24°. Such anatomical conditions make the patellofemoral stabilization lead to compression in the femoro-tibial joint, formation of degenerative changes, meniscus damage, as well as stress on the patellar ligament and its attachment to the tibial tuberosity.
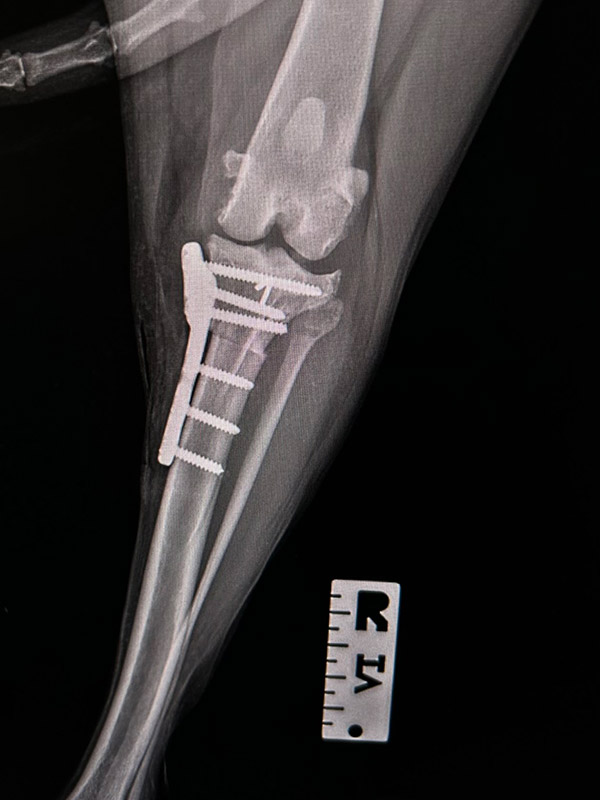
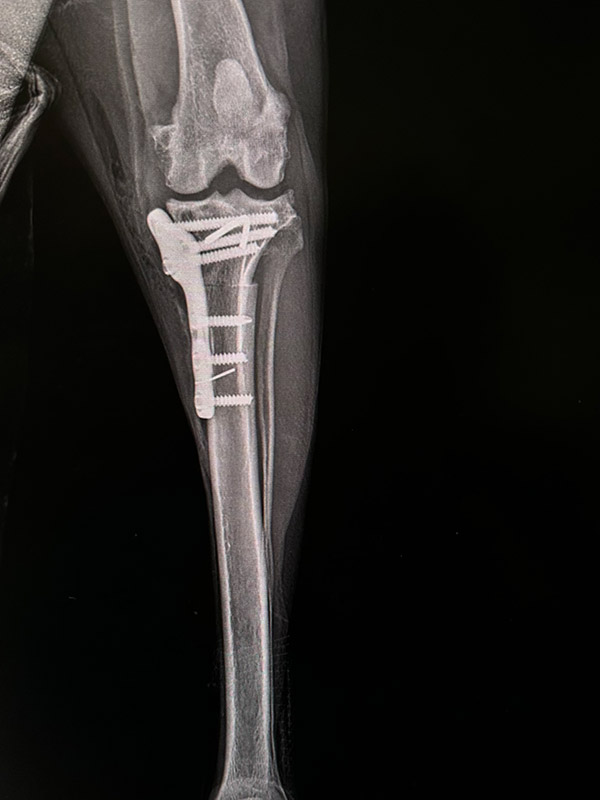
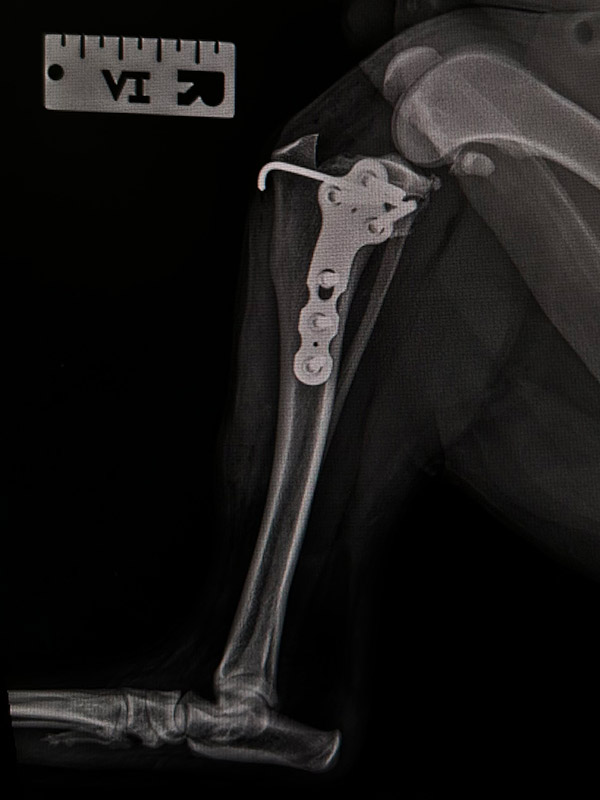
A modification of the TPLO alters the geometry of the angle of the tibial articular plane at its high inclination, allowing for stability in the femorotibial joint.
The procedure of radial tibial osteotomy is performed with the help of an oscillating disc selected adequately to the anatomy of the limb. In miniature breeds, we usually use discs with a radius of R8 or R10 mm. For osteosynthesis after osteotomy, we use a patient-dedicated plate fixed with 1.5 mm diameter locking screws.
TPLO seems to be a simpler method compared to other repair methods. It only takes into account the degree of displacement of the tibial articular plane without having to focus on other considerations, both anatomical and procedural, related to implant selection and acceptance in the healing process.





 This site uses cookies for functional and statistical purposes
This site uses cookies for functional and statistical purposes