
Luxation of the patella is one of the most common orthopedic diseases, occurring in dogs of both large and small breeds.
In veterinary medicine, there are 4 grades of patellar luxation:
- Grade I - where the patella can be luxated during examination, and after pressure is released, it returns to its normal anatomical position,
- Grade II - the patella luxates spontaneously when the stifle is flexed or when it is moved manually, and remains luxated until the limb is straightened at the stifle joint or repositioned by palpation
- Grade III - the patella is luxated, but with pressure we are able to position it correctly, however, after removing the applied force it is luxates again
- Grade IV - the patella is permanently luxated and cannot be restored to its anatomical position
Congenital dislocation of the patella is associated with an anatomical defect consisting in an abnormal location of the tibial tuberosity to which the patellar ligament is attached. The degree of luxation of the patella correlates with the degree of abnormal location of the ligament attachment - the location of the tibial tuberosity.
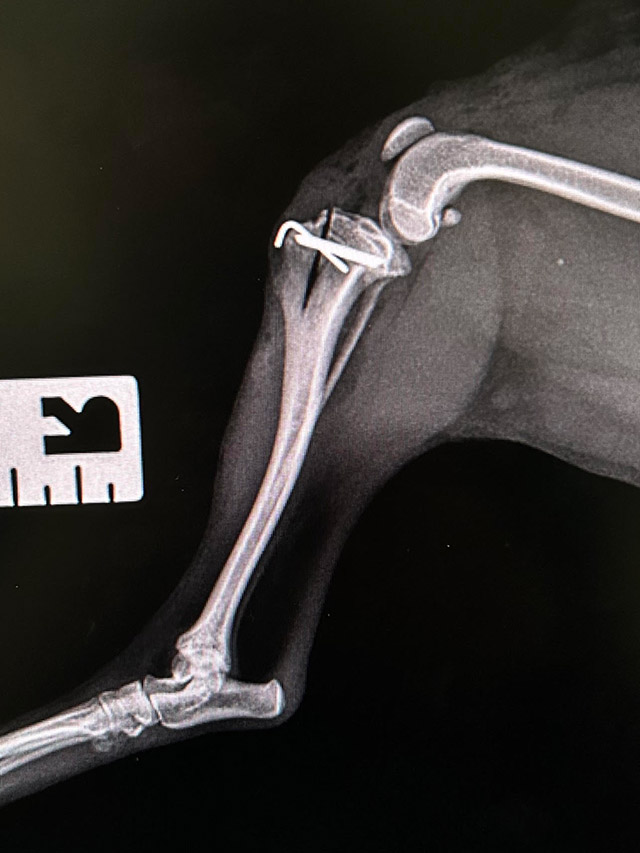
Patient qualification for surgical treatment is carried out on the basis of a clinical examination involving observation of movement, an orthopedic examination of the affected limb and an assessment of the degree of luxation. In the next stage, X-rays are taken in lateral and ventral-dorsal projections.
The TTTT-MTTT- tibial tuberosity transposition technique involves displacement of the tibial tuberosity without its separation from the tibia, and allows for proper function of the patellofemoral joint.
To do this, we perform an osteotomy using an oscillating saw, guiding the cut proximally from the plane of the tibial plateau along the axis of the bone to the area below the curvature of the tibial tuberosity.
In order to spare the tissues surrounding the joint, the last section of the cut is made with a scalpel.
Using a thin wide chisel inserted proximally in the line of the cut, we try to gently release and then, on the principle of the so-called greenstick fracture, bring about the displacement of part of the bone along with the attachment of the ligament to the lateral side. In the case of a young animal, this is a fairly easy procedure and the extent of transfer needed is achieved fairly quickly. In the case of an older patient, heavily calcified bone, this technique requires patience-- too much compression can lead to separation of the bone.
We judge the correct degree of offset of the attachment by the way the patella behaves with flexion and rotation of the limb. A properly preserved mechanism of the muscle prevents the patella from falling out of the intercondylar fossa. If the this cannot be achieved, a medial desmotomy is helpful.
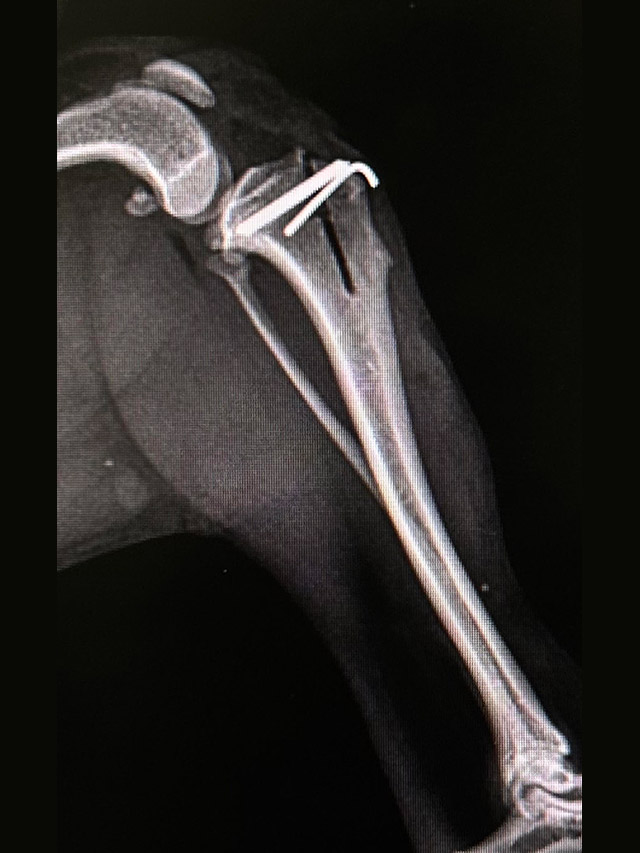
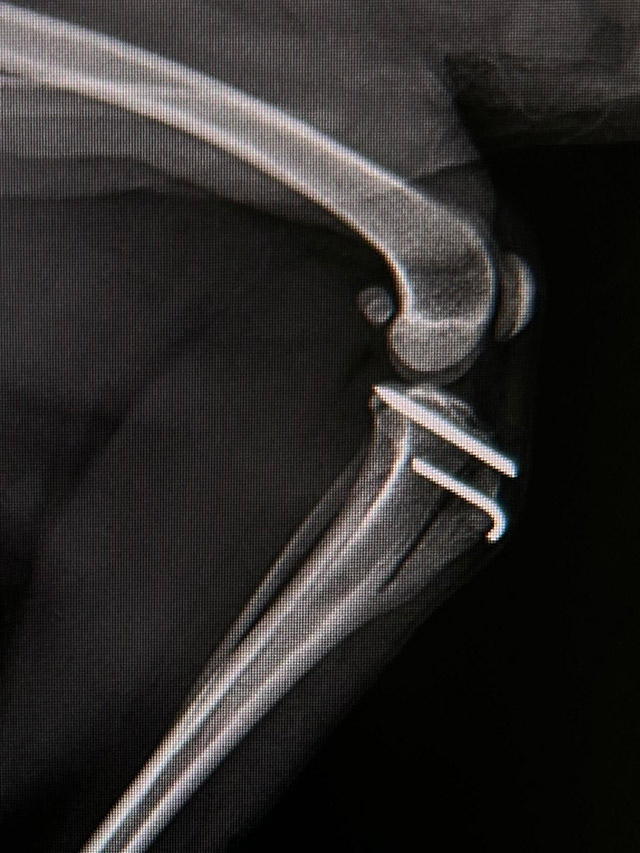
Once the proper degree of displacement is achieved, we stabilize the proper anatomy with an intramedullary nail inserted across the axis of the bone at the beginning of the incision line. It is important that the nail rests against the bone without irritating the ligament.
Additional stabilization is provided by a second thinner nail guided parallel and below the first implant directly through the tibial tuberosity. It is important to bend this nail to avoid irritating the subcutaneous tissue. The wound is then closed by subcutaneous tissue and skin suture. The limb stays in a soft bandage for about a week.
The standard treatment is antibiotics (aminoglycosides or beta-lactams) for about a week.
It is important to use NSAIDs for 3-7 days, as a large percentage of patients are breeds that have a relatively low pain threshold. The use of cool compresses for the first three days after surgery is standard.
The dog begins to bear weight on the limb very quickly, usually as early as the next day.
In the case of miniature breeds, and the most commonly affected patients, even a severe degree of luxation through the use of MTTT along with a desmotomy procedure seems to be a better solution than the standard use of deepening the intercondylar fossa and separating osteotomy of the tibial tuberosity, or attempting to fix the patella with a patellofemoral suture. Wedge trochleoplasty in a miniature patient requires precision and experience.
The MTTT procedure does not resolve all severe degrees of patellar dislocation.
The procedure can be used simultaneously for bilateral patellar luxation due to its low level of trauma.

 This site uses cookies for functional and statistical purposes
This site uses cookies for functional and statistical purposes